
In this guide, you will find practical root cause analysis examples that show how workplace accidents, incidents and near misses can be investigated to identify why they occurred.
We explain the most common root cause analysis methods, when to use them, how to identify immediate, contributing and root causes, and how effective root cause analysis leads to corrective actions that help prevent similar incidents from happening again.
What is root cause analysis?
Root cause analysis (RCA) is the structured process of identifying the underlying reasons why an accident, incident or near miss occurred.
This approach reflects the principles set out in Health and Safety Executive’s Investigating accidents and incidents (HSG245), which recommends identifying immediate, underlying and root causes to learn from incidents and implement effective corrective actions.
Root cause identification
Incidents rarely have a single root cause. Most workplace incidents result from several interconnected root causes, such as weaknesses in procedures, training, supervision, maintenance or communication.
For example, if an employee slips on oil:
- The oil on the floor is not the root cause.
- The leaking equipment, missed inspections and ineffective maintenance programme may all be root causes.
Identifying these underlying issues enables organisations to make lasting improvements rather than simply correcting the immediate problem. This systems-based approach is reflected in James Reason’s Swiss Cheese Model, which explains how incidents often occur when several weaknesses in an organisation’s defences align, rather than as the result of a single mistake.
What is the difference between an immediate cause and a root cause?
The immediate cause is the direct event or hazard that triggered the incident.
The root cause is the underlying failure that allowed the immediate cause to exist.
| Attribute | Immediate cause | Root cause |
| Visibility | Usually obvious at the scene | Often hidden within systems or management arrangements |
| Focus | Explains what happened | Explains why it happened |
| Typical action | Removes the immediate hazard | Improves systems and processes |
| Long-term impact | May prevent one incident | Helps prevent similar incidents recurring |
For example, if a warehouse employee slips:
Immediate cause
Hydraulic oil was present on the floor.
Root causes
- Preventative maintenance was overdue.
- Routine inspections failed to identify the leak.
- Housekeeping responsibilities were unclear.
- Employees had not been trained to report leaks promptly.
Cleaning the spill addresses the immediate cause. Improving maintenance, inspections and reporting procedures addresses the root causes.
What is the difference between a contributing factor and a root cause?
The terms ‘contributing factor’ and ‘root cause’ are often used together, but they mean different things.
A contributing factor increases the likelihood or severity of an incident but may not be the underlying reason it occurred.
A root cause is the underlying failure that allowed the contributing factors and immediate cause to exist.
For example, poor lighting may contribute to a slip, but if housekeeping procedures were ineffective and inspections were not carried out, those management failures are more likely to be the root causes.
Understanding the relationship between immediate causes, contributing factors and root causes helps investigators recommend corrective actions that deliver lasting improvements.
What are root cause analysis methods?
These are examples of root cause analysis techniques commonly used in workplace investigations. The most appropriate method to use depends on the complexity of the incident.
The 5 Whys
The 5 Whys technique repeatedly asks “Why?” until the underlying causes are identified.
This is a simple but effective method for investigating relatively straightforward accidents, incidents and near misses where the sequence of events can be followed logically.
For example:
Problem: Employee slipped.
Why?
There was oil on the floor.
Why?
A hydraulic hose leaked.
Why?
The hose had deteriorated.
Why?
Preventative maintenance was overdue.
Why?
Maintenance planning and scheduling were ineffective.
Rather than stopping at the visible hazard, the investigation identifies weaknesses in maintenance management.
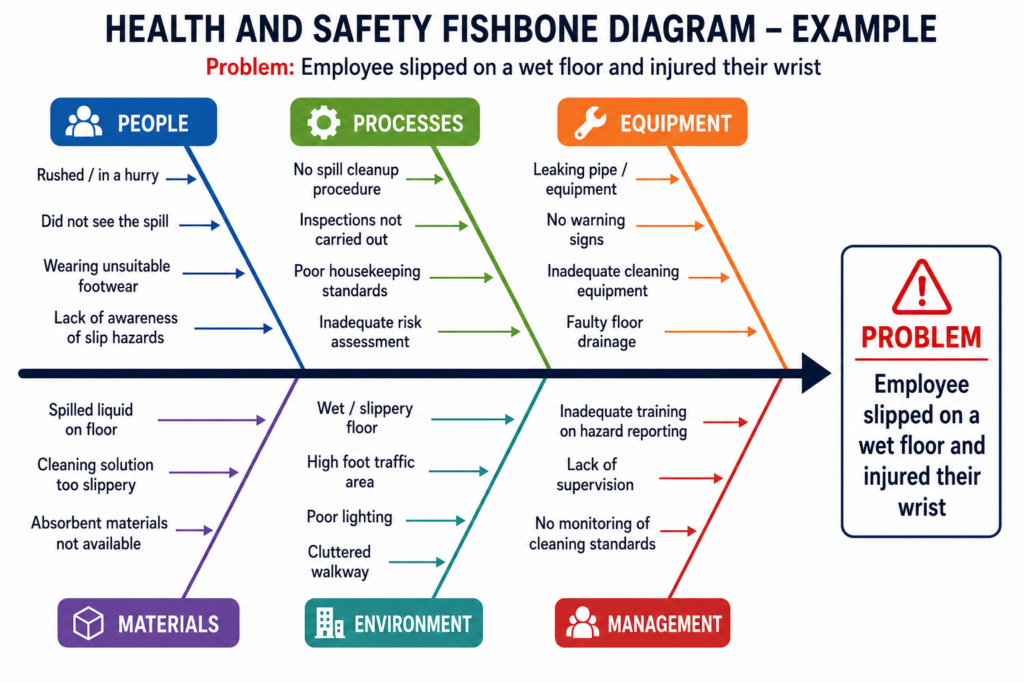
Fishbone (Ishikawa) Diagram
A Fishbone (or Ishikawa) Diagram helps investigators identify and organise all the possible causes of an incident before deciding which are most likely to be the root causes. The incident is written at the “head” of the diagram, while potential causes are grouped into categories such as:
- People
- Equipment
- Methods
- Materials
- Environment
- Management
Investigators then brainstorm the possible causes within each category and use the available evidence to determine which factors contributed to the incident. This structured approach helps ensure that important causes are not overlooked and encourages a broader examination of the systems and processes involved.
A Fishbone Diagram is particularly useful for more complex incidents where there may be multiple interacting causation factors.
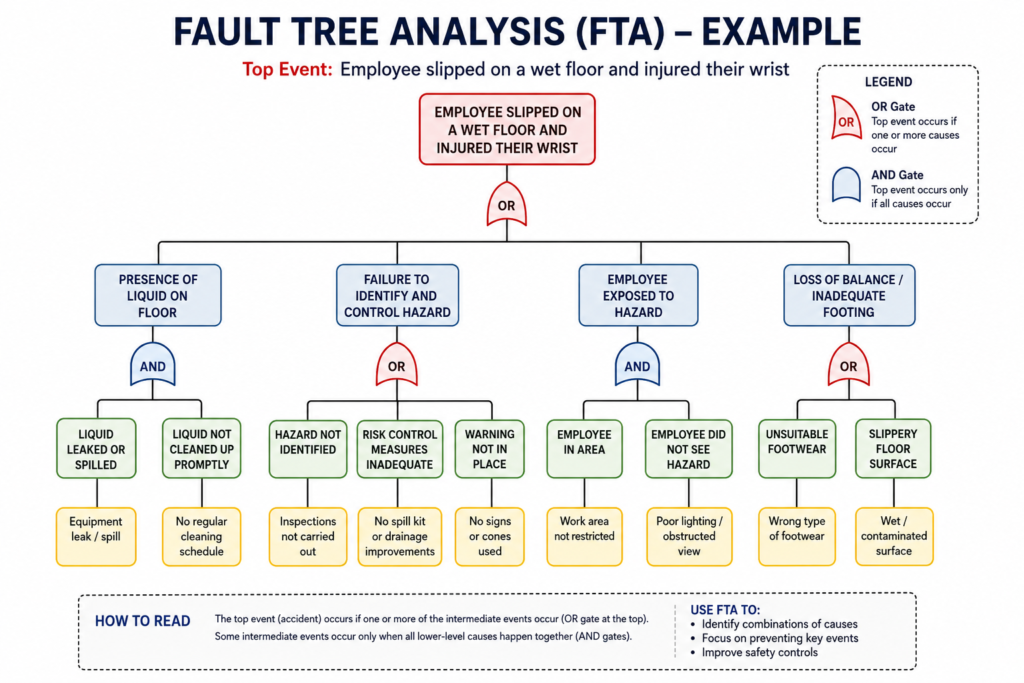
Fault Tree Analysis
Fault Tree Analysis (FTA) is a structured, visual technique used to identify the combinations of failures that could have led to an incident.
Rather than starting by brainstorming all the possible causes, investigators begin with the incident itself (known as the top event) and work backwards, mapping the sequence of failures and conditions that contributed to it using a logical tree structure.
Each branch of the tree represents a failure, condition or event that may have contributed to the incident. These branches are then broken down into increasingly detailed causes until the underlying technical, human and organisational failures are identified. This helps investigators understand not only what went wrong, but also how multiple failures interacted to produce the incident.
Unlike a Fishbone Diagram, which is used to identify and organise potential causes, Fault Tree Analysis focuses on analysing the logical relationships between those causes and how they combined to result in the incident.
This method is particularly useful for complex investigations involving multiple systems or control measures, such as major equipment failures, process safety incidents or high-hazard operations, where there may be many root causes.
What is a timeline analysis?
A timeline analysis reconstructs an incident in chronological order to show exactly what happened before, during and after the event. By arranging the sequence of actions, decisions and events, investigators can identify where controls failed, communication broke down or opportunities to prevent the incident were missed.
Once the timeline has been established, it can then be used alongside other root cause analysis methods to identify the immediate, contributing and root causes.
How do you conduct a root cause analysis?
Although every investigation is different, effective cause analysis generally follows the same structured process.
1. Secure the scene and gather evidence
Protect the area, preserve evidence, take photographs, record environmental conditions and examine equipment before anything changes.
2. Collect witness statements
Interview those involved and anyone who witnessed the incident as soon as possible while events remain fresh. Focus on facts rather than assigning blame.
3. Establish a timeline
Create a clear sequence of events leading up to, during and after the incident. A timeline analysis often reveals gaps in procedures or communication.
4. Identify the immediate and contributing causes
Determine the direct hazards or unsafe conditions that triggered the incident, along with any factors that made it more likely or more severe.
5. Apply root cause analysis techniques
Use appropriate root cause analysis techniques, such as the 5 Whys or Fishbone Diagram, to identify the underlying organisational or management failures.
6. Implement and monitor corrective actions
Corrective actions should address the identified root causes rather than simply removing the immediate hazard. Monitor their effectiveness to ensure the improvements remain effective over time.
When should root cause analysis be carried out?
Root cause analysis should be considered whenever an accident, incident or near miss has the potential to reveal weaknesses in an organisation’s health and safety management arrangements.
Although not every minor incident requires a detailed investigation, organisations should carry out an appropriate level of investigation based on the actual or potential severity of the event. Serious injuries, dangerous occurrences, repeated incidents and significant near misses often justify a formal root cause analysis.
Root cause analysis examples
The following root cause analysis examples show how investigators have identified the underlying causes of workplace incidents and decided on corrective actions.
Example 1: Employee slips on hydraulic oil (5 Whys)
Incident
A warehouse employee slips on hydraulic oil that has leaked onto a pedestrian walkway, fracturing their wrist. The area was not cordoned off, and no warning signs were in place.
Evidence gathered
The investigator:
- Photographs the spill and surrounding area.
- Reviews CCTV footage showing the leak developing over several hours.
- Interviews the injured employee and nearby colleagues.
- Examines maintenance records for the forklift.
- Reviews housekeeping inspection records.
- Checks the workplace risk assessment and spill response procedure.
Investigation findings
The CCTV shows oil dripping from a forklift throughout the morning. Although several employees walked past the leak, it was not reported or cleaned up before the incident occurred. Maintenance records reveal that the forklift’s scheduled inspection was overdue by three weeks.
To understand why the incident occurred, the investigator applies the 5 Whys technique.
| Problem | Employee slipped on hydraulic oil. |
| Why? | Oil had leaked onto the pedestrian walkway. |
| Why? | A hydraulic hose had deteriorated and failed. |
| Why? | Preventative maintenance had not been carried out. |
| Why? | Maintenance schedules were not being monitored effectively. |
| Why? | There was no clear responsibility for tracking overdue maintenance or removing defective equipment from service. |
Investigation outcome
Immediate cause
Hydraulic oil created a slip hazard on the walkway.
Contributing factors
- The leak was not reported promptly.
- Housekeeping inspections had not yet taken place.
- Warning signs or barriers were not used.
- The spill response procedure was not consistently followed.
Root causes
- Preventative maintenance arrangements were ineffective.
- Maintenance responsibilities were unclear.
- Defective equipment remained in use.
- Employees required additional training on spill reporting procedures.
Corrective actions
The organisation:
- Repaired the forklift and inspected similar equipment.
- Introduced an electronic maintenance scheduling system.
- Assigned responsibility for monitoring overdue maintenance.
- Updated the spill response procedure.
- Delivered refresher training on hazard reporting.
- Increased routine workplace inspections.
Rather than simply cleaning the spill, the investigation identified improvements that reduced the likelihood of similar incidents occurring again.
Example 2: Forklift collides with a pedestrian
Incident
A forklift reversing from a loading bay collides with a pedestrian, causing serious leg injuries. The collision occurs during a busy delivery period when several vehicles and pedestrians are moving through the yard.
Evidence gathered
The investigator:
- Reviews CCTV footage.
- Examines the site traffic management plan.
- Interviews the forklift driver, pedestrian and witnesses.
- Reviews driver training records.
- Inspects vehicle maintenance records.
- Examines the workplace layout and signage.
- Reviews recent safety inspection reports.
Timeline analysis
Reconstructing the sequence of events helps identify where opportunities to prevent the incident were missed.
| Time | Event |
| 08:35 | Delivery vehicles begin arriving. |
| 08:42 | Temporary pallets are stored near the loading bay, partially obstructing visibility. |
| 08:46 | The pedestrian leaves the warehouse using the nearest exit rather than the designated walkway. |
| 08:47 | The forklift reverses to collect another load. |
| 08:47 | The driver briefly loses sight of the pedestrian behind the stacked pallets. |
| 08:48 | The collision occurs. |
The timeline shows that several factors combined within a short period rather than a single unsafe act causing the incident.
Fishbone analysis
The investigator then uses a Fishbone Diagram to categorise the possible causes before evaluating which are supported by the evidence.
People
- Pedestrian did not use the designated walkway.
- Driver was unfamiliar with temporary yard changes.
Equipment
- Forklift mirrors provided limited visibility when reversing with a load.
Environment
- Temporary pallet storage obstructed sight lines.
- Increased vehicle movements during deliveries created congestion.
Methods
- Pedestrian and vehicle routes crossed near the loading bay.
- Temporary traffic arrangements had not been communicated effectively.
Management
- The traffic management plan had not been updated to reflect recent operational changes.
- Monitoring of vehicle and pedestrian segregation was inconsistent.
Investigation outcome
Immediate cause
The forklift and pedestrian occupied the same area at the same time.
Contributing factors
- Visibility was obstructed.
- Temporary traffic arrangements increased congestion.
- The pedestrian used a non-designated route.
Root causes
- The traffic management plan no longer reflected how the yard was being used.
- Temporary changes to pedestrian routes had not been communicated effectively.
- Vehicle and pedestrian segregation was inadequate.
- Monitoring of traffic management arrangements was insufficient as site operations changed.
Corrective actions
The organisation:
- Redesigned vehicle and pedestrian routes.
- Installed physical segregation barriers.
- Introduced revised loading procedures during peak delivery periods.
- Updated the traffic management plan following operational changes.
- Improved communication of temporary traffic arrangements.
- Introduced routine reviews of traffic management whenever site layouts changed.
The investigation showed that the collision resulted from a combination of organisational, environmental and operational factors rather than a single mistake by the driver or pedestrian.
Root cause investigation training
Effective root cause analysis requires investigators to gather evidence, identify immediate and underlying causes, evaluate contributory factors and recommend corrective actions that lead to lasting improvements.
Our Incident and Accident Investigation Training provides the practical knowledge and skills to investigate workplace accidents and near misses, apply recognised root cause analysis methods, and work through practical root cause analysis examples that demonstrate how to identify immediate, contributing and underlying causes.
Participants also learn how to produce meaningful investigation reports and implement corrective actions that help prevent similar incidents from happening again.
Find out more about Incident and Accident Investigation Training on our website, or contact our friendly team today on 0203 011 4242 / [email protected]

Adam Clarke
Managing Director (Consulting)
